Non-hereditary Myopathies
Idiopathic inflammatory myopathies
8. Inclusion body myositis
Inclusion body myositis (IBM) is an inflammatory myopathy with onset occurring in middle age or later. Typically, muscles of the anterior thigh and forearm are affected, and this slowly progressive condition is resistant to immunotherapy.
Myopathological features include degeneration and regeneration of muscle fibers with a few showing rimmed vacuoles (Fig. 50) along with predominantly endomysial inflammatory cell infiltrates.
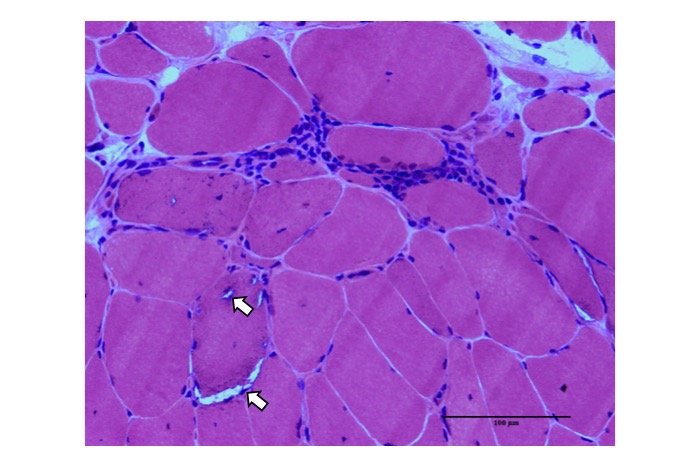
Fig.50
Pathology of inclusion body myositis is characterized by changes of chronic myopathy with rimmed vacuoles (arrows) and inflammation.
Some mononuclear cell infiltrates are observed in contact with the surface of non-necrotic muscle fibers. The infiltrating cells are primarily CD8+cytotoxic T cells, macrophages, and CD4+ cells. Strong aberrant expression of MHC class I antigen is observed on the surface of muscle fibers. Amyloid-positive material, TDP43, p 62, ubiquitinated material, and other proteins that are usually absent in muscle fibers are identified, particularly in muscle fibers containing rimmed vacuoles (Fig. 51).
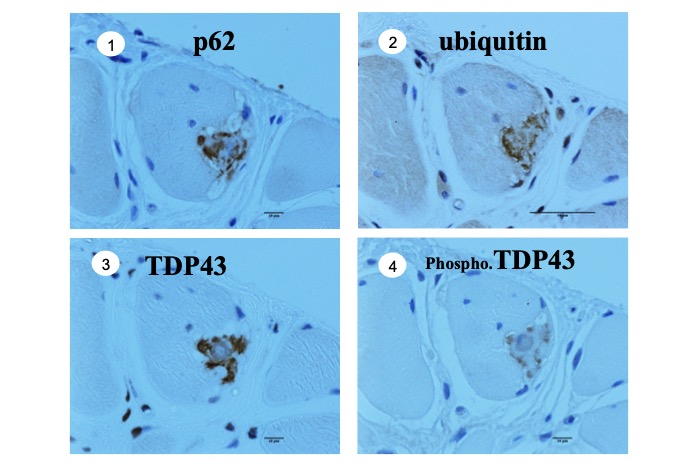
Fig.51
Abnormal deposition of various proteins including p62, ubiquitin, TDP43 and phosphorylated TDP43 are observed, often in the muscle fibers harboring rimmed vacuoles.
Ultrastructural studies reveal autophagic vacuoles containing myelin figures and other debris along with tubulofilamentous inclusions (approximately 20 nm in diameter) (Fig. 52).
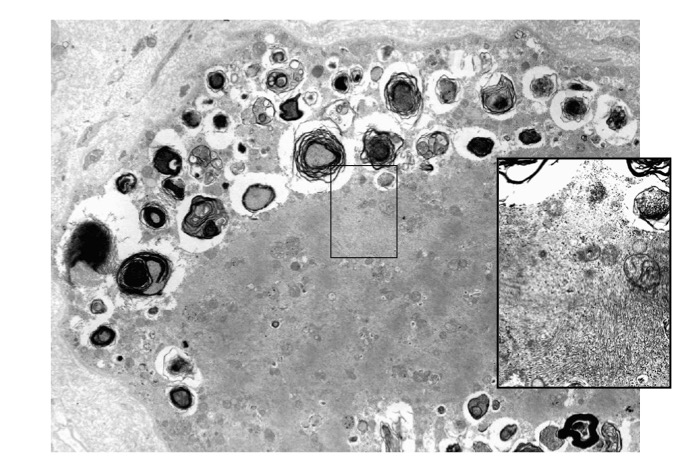
Fig.52
Electron microscopy shows vacuoles containing myelin figures and debris along with tubulofilamentous inclusions, about 20nm in diameter (inset).
Filaments may be visualized within nuclei.
We previously reported disintegration of myonuclear fibrous lamina in the early stages of IBM, which may affect the traffic between the myonucleus and sarcoplasm (Matsubara, 2016c).




