Hereditary myopathies
Congenital myopathies
2. Central core disease
Central core disease shows an AD inheritance pattern. Despite proximal muscle atrophy that occurs in early childhood with delayed motor milestones, most patients retain their ambulatory ability. Skeletal anomalies such as scoliosis, dislocation of the hip and other joints may be observed.
Histopathological findings of muscle tissue include cores in the sarcoplasm with low mitochondrial enzyme activity in these cores. Electron microscopy confirms a paucity of mitochondria in the core (Fig.27).
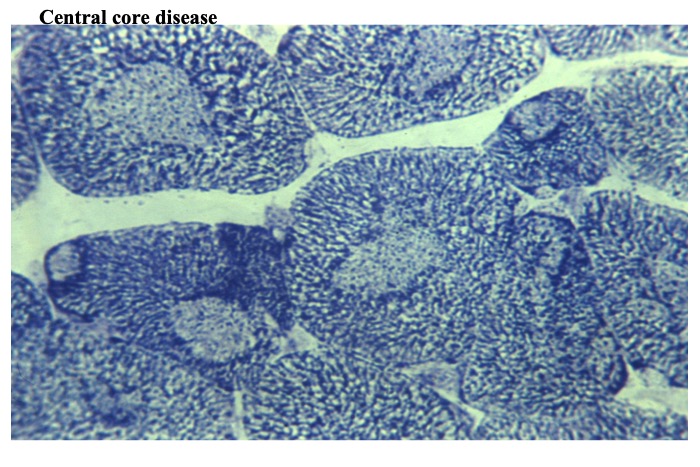
Fig.27
Central core disease (NADH-TR activity)
Cores appear like target fibers. However, they often lack a band of high activity of mitochondrial enzymes around a central area of low activity. The cores run longitudinally for a considerable distance along the muscle fibers, whereas target fibers extend over short distances. Ultrastructurally, the cores contain few mitochondria and show deranged myofibrils such as Z-line streaming.
Ryanodine receptor 1 (RYR1) is a calcium ion channel located in the sarcoplasmic reticulum that responds to electrical excitation caused by the T tube by releasing Ca2+ as part of excitation-contraction coupling. Some cases of multi-minicore myopathies might show mutations in RYR1. Nemaline rods can be seen in association with central cores. Although most cases of central core diseases are related to mutations in RYR1, a small number of cases related to mutations in skeletal α-actin 1 (ACTA1), titin and other genes have been reported.




