Non-hereditary Myopathies
Idiopathic inflammatory myopathies
7. Immune-mediated necrotizing myopathies
The concept of immune-mediated necrotizing myopathy has evolved following the discovery of inflammatory myopathies associated with a few autoantibodies that are closely associated with myopathy categorized as necrotizing myopathy with no or little inflammation. However, the etiopathogenetic role of autoantibodies in these myopathies remains unclear.
(1) Anti-signal recognition particle (SRP) antibody-associated necrotizing myopathy
SRP is a multifunctional protein in the endoplasmic reticulum that participates in the transfer and degradation of proteins. An autoantibody against SRP was detected in the sera of 4–8% of patients with inflammatory myopathy (Targoff, 1990; Suzuki, 2008). These patients often show an unfavorable response to the usual immune therapy administered for myositis. Histopathological findings in muscle specimens are characterized by scattered necrotic fibers with sparse or no inflammatory cell infiltrates often showing weak or no aberrant expression of the MHC class I antigen on the surface of muscle fibers (Fig. 48).
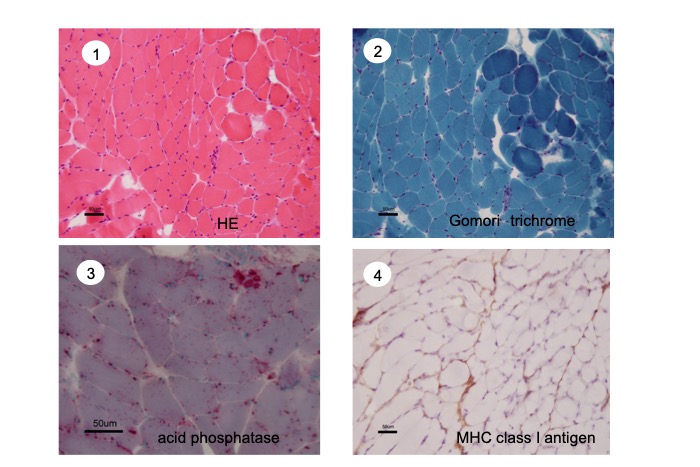
Fig.48
Immune mediated necrotizing myopathy with anti-signal recognition particle (SRP) antibody. ① HE, ② TC, ③ acid phosphatase, ④ MHC class I antigen.
Many necrotic fibers with positive acid phosphatase are present, but little sign of inflammation is seen. Aberrant expression of MHC class I antigen is weakly detected on the surface of muscle fibers.
Association with collagen vascular disease is uncommon in these patients. Serum muscle enzyme levels are usually high (serum CK is often >1,000 IU/L). Although patients are usually refractory to immune therapy, intravenous immunoglobulin administration may be effective in some patients.
(2) Anti-3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMGCR) antibody-associated necrotizing myopathy
HMGCR is anchored in the membrane of the endoplasmic reticulum and shows eight transmembrane domains. It plays a key role as the rate-controlling enzyme in the mevalonate pathway that is essential for the production of cholesterol and other terpenoids. It is the target of statins, (cholesterol-lowering drugs), and hyper-CKemia and muscle impairment are commonly known adverse effects of this class of drugs. A study has shown that these adverse effects continued to progress in a small percentage of patients despite discontinuation of statins (Neeham, 2007). Subsequently, an antibody against HMGCR was detected in some of these patients (Mammen, 2011). Furthermore, this antibody was positive among patients with weakness or hyper-CKemia even without a history of statin intake (Mohassel, 2013).
Histopathological findings in muscle specimens show necrotizing myopathy with little or no inflammatory cell infiltration. Aberrant expression of the MHC class I antigen is usually noted on the surface of muscle fibers (Chung, 2015) (Fig. 49), although this may be absent.
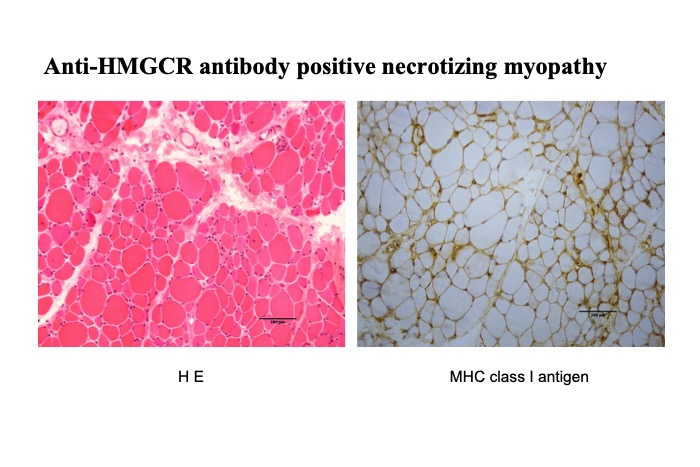
Fig.49
Myopathic changes without inflammation were seen on HE stain, but a moderate degree of aberrant expression of MHC class I antigen suggested a possibility of inflammatory myopathy. This patient was treated for myositis for 20 years before anti-HMGCR antibody was found positive.
An association with malignancy is reported to be common (Limaye, 2015; Tsujikawa, 2016). We previously reported mitophagy in three cases of IMNM with positive anti-HMGCR antibody (Matsubara, 2018).




