Non-hereditary Myopathies
Idiopathic inflammatory myopathies
2. Dermatomyositis
Cutaneous changes associated with dermatomyositis (DM) include a heliotrope rash and the Gottron’s, shawl, and V-neck signs. These represent the Koebner phenomenon, which occurs secondary to repeated physical stimulation of the skin.
Histopathological findings include inflammatory cell infiltrates distributed predominantly in the perifascicular area and the perimysium or perivascular region. Muscle atrophy caused by degeneration and regeneration is primarily noted in the perifascicular region resulting in “perifascicular atrophy” (Fig.44), which is important for the histopathological diagnosis of DM (Table 6). Inflammatory cells are predominantly CD4+ cells.
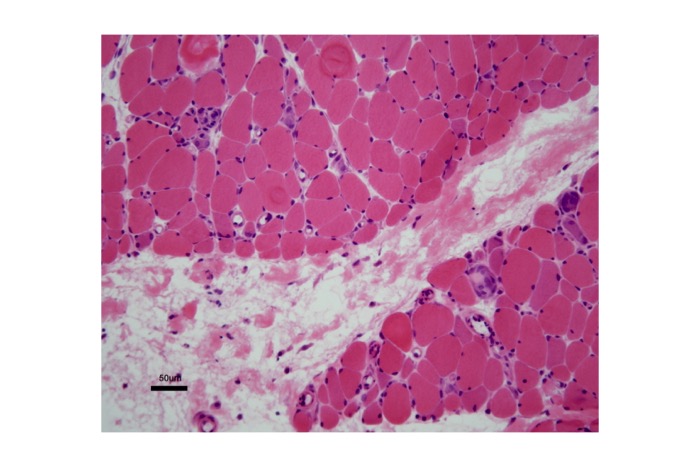
Fig.44
A muscle biopsy of a patient with dermatomyositis showing perifascicular atrophy.
Diagnostic criteria for dermatomyositis (Dalakas and Hohlfeld, 2003)
| diagnosis | Myopathic dermatomyositis | Amyopathic dermatomyositis | |
| definite | probable | ||
| weakness due to myopathy | yes | yes | no |
| electromyography | myopathic | myopathic | myopathic or non-specific |
| muscle enzyme (eg. serum-CK ) | high (up to 50 times normal)or normal | high | high (up to 10 times normal)or normal |
| muscle biopsy | perifascicular・perimysial or perivascular Infiltrates; perifascicular atrophy | perifascicular・perimysial or perivascular Infiltrates; perifascicular atrophy | Non-specific or diagnostic for dermatomyositis (subclinical myopathy) |
| skin change or calcificaiton | present | not detected | presnt |
Tab.6
Abundant macrophages and CD20+B cells are also present (Fig. 45).
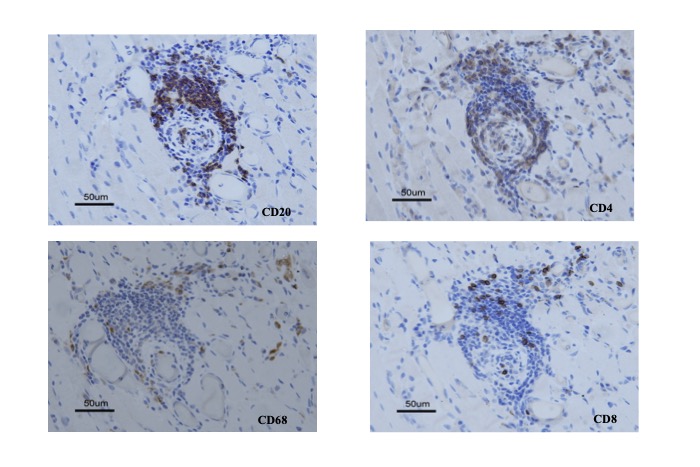
Fig.45
Subset of inflammatory cells in the muscle of a patient with dermatomyositis. CD20+ B cells, CD4+T cells, CD68+ macrophages and CD8+T cells are observed.
Aberrant expression of the MHC class I antigen is usually prominent in the perifascicular fibers. Many of the perifascicular fibers are type 2C fibers representing regenerating fibers. Necrosis en masse of muscle fibers may be observed in severe cases of DM.
The membrane attack complex or C5b-9 is often identified on the walls of blood vessels in tissue obtained from patients with DM in addition to a reduction in the number of blood vessels (Emslie-Smith, 1990). Ultrastructural examination may reveal granulotubular inclusions and rod-shaped bodies (Weibel-Palade bodies), as well as filamentous inclusions in the cytoplasm of the endothelial cells of blood vessels in muscles. However, these inclusions can occur even in other collagen vascular diseases. The association between atrophic muscle fibers, perimysial inflammation and changes in blood vessels remain unclear. Roles played by various cytokines associated with inflammation might be important.
Cutaneous manifestations often precede muscle symptoms in cases of juvenile dermatomyositis (JDM), which by definition occurs in the pediatric population. Interstitial lung disease needs careful evaluation in all patients, because it may initially occur as a subclinical condition with subsequent aggravation. Cutaneous manifestations resemble those observed in adult cases of DM. Weakness is commonly observed in the hip, shoulder girdle and neck muscles. Myalgia sometimes causes contracture of joints as children avoid limb movements. Bulbar muscles can be affected in severe cases. Histopathological examination of muscle specimens in cases of JDM is characterized by prominent vasculitic changes and massive collections of necrotic fibers that are sometimes accompanied by calcification. Perifascicular atrophy is observed and dense inflammatory cell infiltrates are noted, particularly perivascular in distribution.




