Non-hereditary Myopathies
Idiopathic inflammatory myopathies
Discovery of new conditions in recent years has made classification of inflammatory myopathies somewhat fluid. Following conditions are to be described (Table 4).
Inflammatory myopathies
- Polymyositis
- Dermatomyositis
Including:- Clinically amyopathic dermatomyositis
- Childhood (or Juvenile) dermatomyositis
- Anti-synthetase syndrome induced dysimmune myopathy
- Overlap syndrome
- Non-specific myositis
- Cancer associated myositis
- Immune-mediated necrotizing myopathies
- Anti-signal recognition particle antibody associated necrotizing myopathy
- Anti-HMG CoA reductase antibody associated necrotizing myopathy
- Inclusion body myositis
- Other inflammatory myopathies
- Granulomatous myopathies including sarcoid myositis
- Focal myositis
- Eosinophilic myositis
- Myositis due to graft vesus host disease
- Adult-onset nemaline myopathy
Tab.4
1. Polymyositis
According to the diagnostic criteria proposed by Bohan and Peter (1975 a,b), absence of skin rash is the sole criterion that distinguishes polymyositis (PM) from dermatomyositis(DM). PM and DM predominantly affect proximal muscles associated with elevated serum CK level. However, heterogeneous inflammatory myopathies without skin rash have been recognized since the introduction of these criteria and newer concepts have emerged regarding the understanding of PM. In this section, we discuss PM from a pathological viewpoint.
Since Arahata and Engel (1989) published their study, the Dalakas and Hohlfeld (2003) (Tables 5, 6) diagnostic criteria were established for PM and DM, followed by guidelines recommended by the European Neuromuscular Center (De Bleecker, 2015). These guidelines define PM as a condition in which CD8+ cytotoxic T cells attack and destroy muscle cells, which aberrantly express MHC class I antigen on their surface. This implies that muscle biopsy and immunohistochemical studies are needed to diagnose a patient with PM. Diagnosing patients with PM based on these criteria (Table 5)was challenging in clinical practice. We perform MRI before muscle biopsy in patients with inflammatory myopathies to obtain a muscle specimen showing inflammation.
Diagnostic criteria for polymyositis (Dalakas and Hohlfeld,2003)
| diagnosis | polymyositis | |
| definite | probable | |
| moypathic muscle weakness | yes | yes |
| electromyographic findings | myopathic | myopathic |
| muscle enzyme(eg. serum-CK ) | high (up to 50 times normal) |
high (up to 50 times normal) |
| Muscle-biopsy findings | primary inflammation with CD8/MHC-1 complex, no vacuole | Ubiquitous MHC-1 expression, no CD8+ expression, no vacuole |
| rash or calcificaiton | absent | absent |
Tab.5
However, PM was still identified only in a limited number of patients among those who underwent muscle biopsy and immunohistochemical investigations.
In PM, muscle samples typically show non-necrotic muscle fibers surrounded and contacted by CD8+ cytotoxic T cells (Fig. 42).
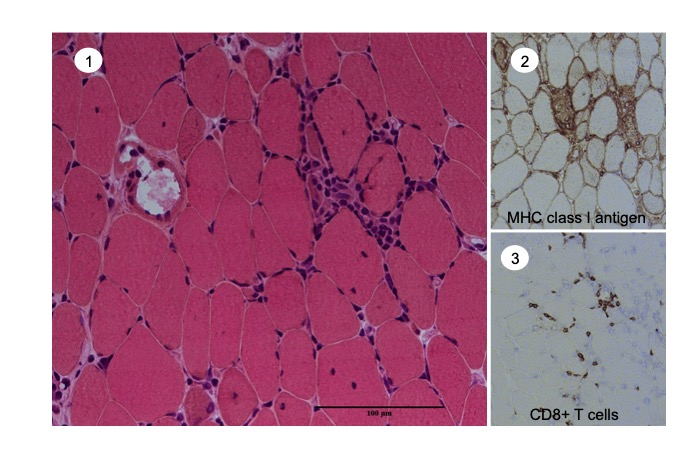
Fig.42
Polymyositis ① Inflammatory cell infiltration in the endomysium (HE) ,② Aberrant expression of MHC class I antigen on the surface of muscle fibers; expression was also seen on many of the infiltrating cells, ③ CD8+ cells in contact with the muscle fibers including non-necrotic fibers.
CD4+ cells are often present in the vicinity along with macrophages. CD4+ cells control both Th1 and Th2 cells; therefore, their presence does not exclude a diagnosis of PM.
Another diagnostic challenge is accurate verification of CD8+ cell-mediated injury to non-necrotic sections of the muscle fiber. The entire stretch of a muscle fiber does not undergo simultaneous necrosis, and muscle injury is an ongoing process. Therefore, it is difficult to confirm whether a fiber is necrotic based on examination of a transverse section. Necrotic fibers may or may not be infiltrated by macrophages, which are often used as markers of necrotic activity in a muscle fiber. Infiltration of macrophages does not conclusively prove necrosis of the fiber, and fairly well-preserved muscle fibers infiltrated by macrophages may be observed in myopathies. Furthermore, it is often difficult to confirm cytotoxic T cell contact to muscle fibers. Electron microscopy is needed to know whether the lymphocyte is located outside of the basal lamina of the muscle fiber or under the basal lamina in direct contact with the plasma membrane of the muscle fiber (Fig. 43).
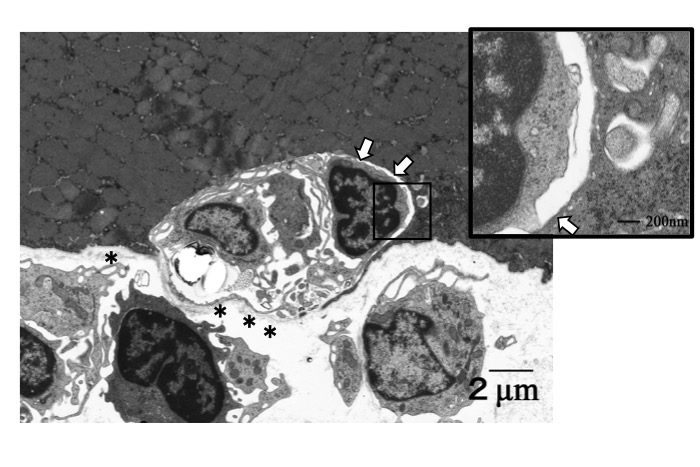
Fig.43
Electron microscopic observation of polymyositis. Three inflammatory cells are seen underneath the basal lamina (stars) of a non-necrotic muscle fiber. A mononuclear cell is in direct contact with the surface of the muscle cell (arrows).




